History Taking and Progres Note (SOAP Notes)
Source: https://www.ncbi.nlm.nih.gov/books/NBK482263/
Introduction
History taking is an essential skill for medical practitioners. There are many ways to document patient complaints. I personally use SOAP Note to record patient histories. Larry Weed created this system almost 50 years ago. It is a widely used documentation method for healthcare providers. SOAP stands for
- Subjective
- Objective
- Assessment
- Plan
Subjective (Symptoms)
Comes from the “subjective” experiences, personal views or feelings of a patient or someone close to them. In the inpatient setting, interim information is included here.
-
Chief Complaint (CC) Examples: chest pain, decreased appetite, shortness of breath.
- History of Present Illness (HPI)
Example: 47-year old female presenting with abdominal pain.
This is the section where the patient can elaborate on their chief complaint. An acronym often used to organize the HPI is termed “OLDCARTS”:
- Onset: When did the CC begin?
- Location: Where is the CC located?
- Duration: How long has the CC been going on for?
- Characterization: How does the patient describe the CC?
- Alleviating and Aggravating factors: What makes the CC better? Worse?
- Radiation: Does the CC move or stay in one location?
- Temporal factor: Is the CC worse (or better) at a certain time of the day?
- Severity: Using a scale of 1 to 10, 1 being the least, 10 being the worst, how does the patient rate the CC?
- History
- Medical history: Pertinent current or past medical conditions
- Surgical history: Include the year of the surgery and surgeon if possible.
- Drug history: Current and past drugs/medication.
- Family history: Include pertinent family history. Avoid documenting the medical history of every person in the patient’s family.
- Social History: HEADSS which stands for Home, Education/Employment, Activities, Drugs, Sexuality, and Suicide/Safety
- Review of Systems (ROS)
- General: Weight loss, decreased appetite
- Gastrointestinal: Abdominal pain, hematochezia
- Musculoskeletal: Toe pain, decreased right shoulder range of motion
Objective (Sign)
This section documents the objective data from the patient encounter. This includes:
- Alert, conscious
- Vital signs
- Physical exam findings
- Laboratory data
- Imaging results
- Other diagnostic data
- Recognition and review of the documentation of other clinicians.
Assessment
This section documents the synthesis of “subjective” and “objective” evidence to arrive at a diagnosis. This is the assessment of the patient’s status through analysis of the problem, possible interaction of the problems, and changes in the status of the problems. Elements include the following.
-
Problem List the problem list in order of importance. A problem is often known as a diagnosis.
-
Differential Diagnosis This is a list of the different possible diagnosis, from most to least likely, and the thought process behind this list. This is where the decision-making process is explained in depth. Included should be the possibility of other diagnoses that may harm the patient, but are less likely.
Plan
This section details the need for additional testing and consultation with other clinicians to address the patient’s illnesses. It also addresses any additional steps being taken to treat the patient. This section helps future physicians understand what needs to be done next.
Extra
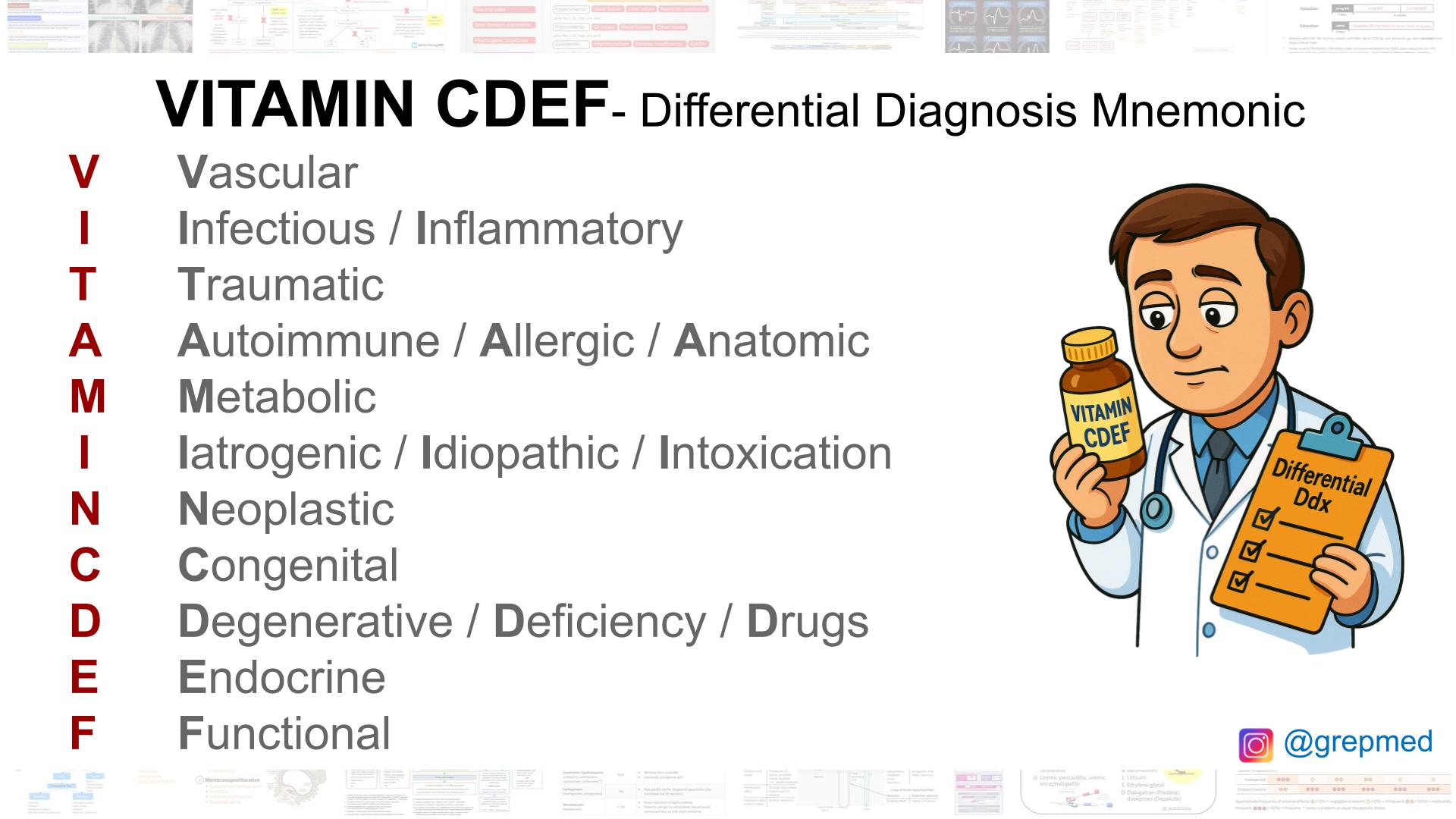 DDX Mnemonic
DDX Mnemonic